By Javier Fernández Ruiz

Javier Fernández Ruiz holds a PhD in Biology (1986) from the Complutense University of Madrid (UCM). He is currently a professor in the UCM's School of Medicine. He has been working as a researcher for the last 36 years and has written many research articles and chapters for books. He has filed 5 patents. He lectures in universities, research centres and at conferences. He is currently the principal investigator of the CANNABINOIDS-BBM3 research group of the University Institute of Research in Neurochemistry at the UCM, the CIBERNED, and the IRYCIS. The group's work centres on the study of the therapeutic potential of cannabinoids in various neurodegenerative diseases. It collaborates with several Spanish and international groups. Dr Fernández Ruiz has been principal investigator on 26 research projects. He was the president of the "International Cannabinoid Research Society (ICRS)" from 2002-2003 and was a founding member of the Spanish Cannabinoid Research Society (SEIC), of which he has been the Secretary (2000-2007) and President (2007-2011). He currently sits on the governing board of the IRYCIS, the scientific advisory board of the company VivaCell Biotechnology Spain and the editorial committee of the British Journal of Pharmacology.
Cannabinoids and neurodegenerative disorders
One of the most promising and currently more investigated therapeutic properties of cannabinoids is their ability to preserve neurons and other neural cells against those neurotoxic stimuli that damage their homeostasis, integrity and survival during neurodegenerative processes.
Such neuroprotective benefits have been found in numerous studies carried out during the last 20 years in preclinical models of stroke, brain trauma, spinal injury, or in chronic progressive neurodegenerative disorders, such as Alzheimer's disease, Parkinson's disease, amyotrophic lateral sclerosis, Huntington's chorea and other pathologies, and eventually in a few clinical studies, including the use of medicinal cannabis, carried out in patients suffering these disorders.
Despite these results, the expectation is that the way towards having approved cannabinoid-based medicines for the treatment of these disorders will be still long, and will require, among others, the identification of the best targets for cannabinoids to exert their neuroprotective effects, the study of their synergies given the need to work with broad-spectrum therapies, and the optimization of the cannabinoid-based treatments for each disorder.
Anyway, the hope recruited by current preclinical and clinical data obtained in the different neurodegenerative disorders supports the need to move the issue towards the clinical scenario, which results essential by the following three reasons:
- Neurodegenerative disorders will become epidemic in the XXI century given the expected increase in the world population, in particular people over 65 year-old, as well as the expected elevation in lifespan that will give more possibilities to these disorders to be visible.
- Current licensed neuroprotective therapies for neurodegenerative disorders are scarce and they have limited efficacy, leaving these disorders as the major biomedical challenge for translational research in the present century.
- There is a progressively growing interest in cannabinoids and medicinal cannabis for the treatment of human pathologies, in particular for those in which current clinical outcome is poor, which represent one of the most attractive niches for moving cannabinoid/cannabis-based therapies from the present preclinical research towards the clinical scenario, and this is the case of neurodegenerative disorders.
The case of amyotrophic lateral sclerosis
One of the most interesting neurodegenerative disorders in terms of progression in cannabinoid research is amyotrophic lateral sclerosis (ALS). This disease, also called Lou-Gehrig's disease in USA or Motor Neuron Disease (MND) in UK, is an aggressive and fastly-progressing disorder with an incidence of 1.5-2.7 cases per 100.000 subjects. However, the prognosis after ALS diagnosis is short (3-5 years), which means that prevalence is ALS is approximately 5.2 cases per 100.000 subjects. Upper and lower motor neurons, which are responsible of the control of voluntary and conscious movement, as well as the skeletal muscles controlled by lower motor neurons, are the major targets of the degenerative process in ALS, which occurs by a combination of several neurotoxic insults that are summarized in the following figure and that results in muscle denervation, weakness and atrophy leading lastly to paralysis and death frequently by respiratory failure:
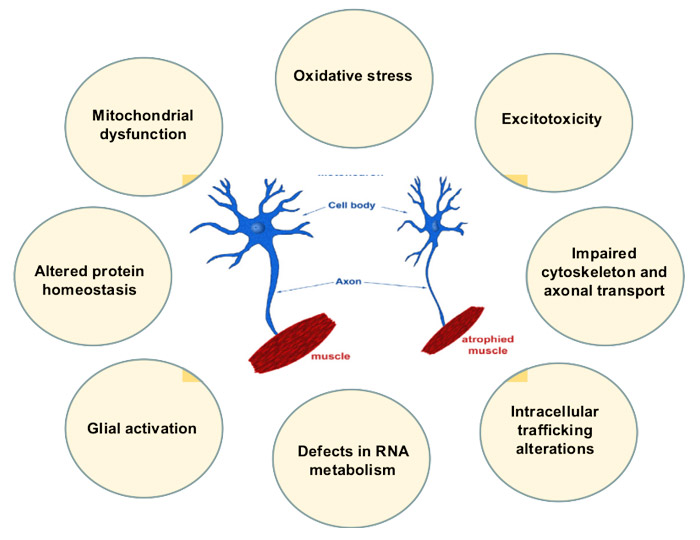
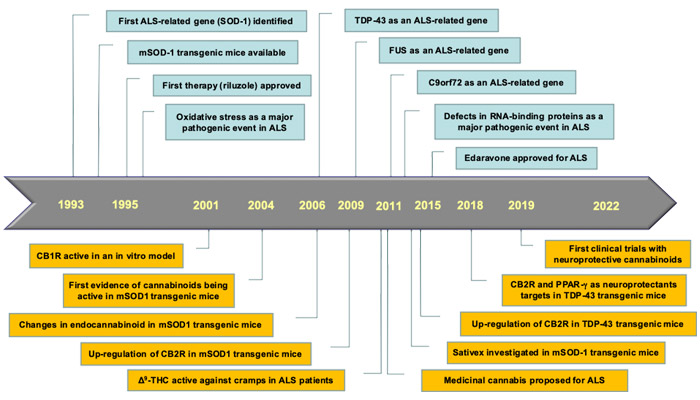
In 20% of patients, the disease is originated because mutations in one of more than 25 different genes already identified in relation with ALS. These cases are classified as familiar ALS (fALS), whereas the disease in approximately 80% of patients is due to the combination of different environmental factors being classified as sporadic ALS (sALS). The predominant affectation of upper and lower motor neurons and skeletal muscles means that major symptoms in ALS are related to muscle atrophy, so that ALS was classically considered as a motor disorder predominantly associated with alterations in the gene encoding the antioxidant enzyme Superoxide dismutase-1 (SOD-1), which was the first ALS-related gene identified in 1993. However, against the classic idea that cognition is not affected in ALS patients and that they are always terribly conscious of their progressive and fast deterioration, a series of new discoveries including the identification of some new ALS-related genes encoding the RNA-binding proteins TAR-DNA–binding protein-43 (TDP-43), Fused in sarcoma (FUS), and Chromosome 9 open reading frame 72 (C9orf72), most of them occurring in the beginning of the present century, have modified the interpretation of ALS as a simply motor disorder caused by excessive oxidative stress. Therefore, against those patients having mutations in SOD-1 gene, which develop a classic disease phenotype characterized by motor defects, those patients having mutations in TDP-43, FUS, C9orf72 and other recent genes present a phenotype combining both motor and cognitive problems. The discovery of these new genes also promoted a change in the interpretation of the major pathogenic events in ALS, evolving from the traditional view of ALS, as a disorder having a predominant influence of oxidative stress due to mutations in SOD-1, to new views that put the emphasis in defects in RNA metabolism due to mutations in RNA-binding proteins TDP-43, FUS and C9orf72, together with additional genes whose mutations affect protein homeostasis. The chronology of these discoveries is presented in the next figure, in parallel to the chronology of main advances in relation with the potential of cannabinoids as an ALS therapy, which will be described in the following paragraphs:
Cannabinoid-based therapies in development for ALS
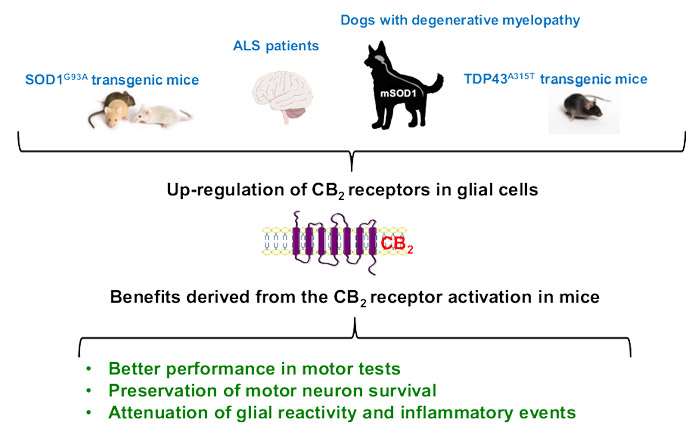
Despite the efforts addressed to develop effective treatments able to alleviate specific symptoms (e.g. cramps, spasticity) or to delay disease progression, ALS still lacks an effective therapy. At present, the antiexcitotoxic agent riluzole (Rilutek®), approved in 1995, and the antioxidant compound edaravone (Radicava®), approved in 2015 in Japan, 2017 in USA and 2018 in Canada, are the only available medicines for patients, and both have only modest effects on disease progression. Due to these limited treatment options, numerous new compounds and other strategies are currently under preclinical and clinical investigation. An interesting option is cannabinoids, which have recently been proposed as a promising multitarget strategy for ALS following their effects in other neurodegenerative disorders. This proposal comes from the results generated in a series of consecutive preclinical studies initiated in the beginning of the present century (see the above figure for a chronological view), which were addressed to investigate different cannabinoids for their neuroprotective effects in ALS. Mary Abood's laboratory* contributed significantly to these initial studies demonstrating for the first time the efficacy of activating CB1 receptors in an in vitro model of ALS, studies that were followed by in vivo data obtained in the classic mutant SOD-1 mouse model, but also in new models mainly based on TDP-43 protein, with different types of plant-derived or synthetic cannabinoids. These experiments demonstrated the relevance of targeting the CB2 receptor and also the PPAR-γ receptor. In the case of CB2 receptors, these studies followed previous research that demonstrated elevations in the levels of the CB2 receptor in glial cells in the spinal cord in ALS patients and animal models, as indicated in the following figure:
In this sense, pharmacological (treatment with selective CB2 receptor agonists and antagonists) and genetic (ablation of the CB2 receptor gene in experimental ALS) studies carried out in our laboratory using TDP-43 transgenic mice have situated the CB2 receptor as an important and promising target (alone or combined with CB1 and/or PPAR-γ activators) to develop a disease-modifying therapy in ALS, which we expect to be able to move towards the clinical scenario in the next years. Meanwhile, other initiatives with cannabinoids in ALS have already arrived the clinical scenario, for example the clinical trial conducted in Switzerland with Δ9-THC for cramps in ALS, which reported some benefits, and the more recent and still ongoing clinical trials (MediCabilis and EMERALD) which explores the disease-modifying benefits of standardized cannabis extracts in cohorts of ALS patients.
Our expectation is that more clinical trials will follow, including selective CB2 agonists, with the objective to license cannabinoid-based therapies for patients affected by a terrible disease with no cure and limited therapeutic outcome at present.
*Mary Abood passed away in past February, so this mention is an homage to her great contribution to the progress of cannabinoids as therapies for ALS patients


