By Guillermo Moreno-Sanz

Dr. Moreno-Sanz has authored more than 30 scientific articles and 3 patents describing the role of the endocannabinoid system in pain perception. Graduated in Biochemistry and Organic Chemistry from the University of Zaragoza, he obtained his PhD in Neuroscience from the Complutense University of Madrid, in Spain. He gained extensive international experience with long-term fellowships in the Netherlands, Italy, and the United States, developing most of his academic career at the University of California, Irvine, where he discovered a new class of cannabinoid analgesic with high clinical potential. In 2017, he acted as a consultant to the National Academies of Sciences of the United States in the preparation of the report "The health effects of cannabis and cannabinoids" and later founded Abagune Research to offer scientific advice and R&D solutions to the international cannabis industry. In 2020 he assumes the scientific and medical direction of Khiron Life Sciences in Europe.
A rat is not a monkey is not a human.
It was 2012 when pharmaceutical giant Pfizer published the results of its Phase II clinical trial investigating the efficacy of the molecule PF-04457845, an inhibitor of the degradation of the endocannabinoid anandamide, in osteoarthritis patients with chronic knee pain. The results of the trial indicated that this potent inhibitor of the enzyme FAAH was able to increase endocannabinoid levels but patients did not report an analgesic effect superior to that of ibuprofen, which was used as control.1
This result was a disappointment for all of us working on the development of this type of compounds, which represented the most promising clinical candidates for a drug capable of exploiting the endocannabinoid system clinically since its discovery in the 1990s. For me, who had been working on a similar group of drugs for four years, the result was both disappointing and intriguing. It is well known that a vast majority of compounds that work well in animal models fail when they reach the clinic. However, the fact that FAAH inhibitors have shown efficacy in animal models of pain of very different nature (nociceptive, inflammatory, neuropathic, etc.) together with the real-world evidence confirming, time and again, the widespread use of medical cannabis for chronic pain relief, made this technology very promising for developing a new class of analgesics with a favorable safety profile. Once the result was digested, the scientific community began to question the rationale behind Pfizer's result. One of the pioneers of anandamide pharmacology, Vincenzo Di Marzo, explored in an editorial very much in his style different reasons why pain control through stimulation of the endocannabinoid tone might not be as fa(ah)cile as initially expected.2 One of the main arguments Di Marzo made in his commentary was that cannabinoids had demonstrated efficacy in chronic pain conditions in which patients had a higher degree of anxiety. Even the Pfizer trial investigators suggested that the low affective component of the model used may have contributed to the lack of efficacy demonstrated by PF-04457845. This reminded me of a review I had read a couple of years earlier when I was a predoctoral student, in which experts in the neurological processing of pain explained that rats and other lower mammals simply do not possess the neuroanatomical structures responsible for pain processing in humans.3 I didn't pay much attention to it at the time because I was in the final stretch of my PhD and the last thing you want to think about before defending your thesis is the real utility of what you are doing. But since I started working with patients using medical cannabis, this modulatory effect of the endocannabinoid system on the affective component of chronic pain has become one of the keys to explaining the responses observed in clinical practice.
Pain intensity, pain threshold and suffering.
Current evidence clearly indicates that the experience of chronic pain in humans is composed of both sensory and affective dimensions, and is often accompanied by the desire to end, reduce, or escape from it. This affective dimension of pain is partly made up of emotions referring to the patient's present or short-term future, such as distress or fear. Another affective component of pain, the "secondary affect" is composed of feelings motivated by the long-term implications of having chronic pain, such as suffering. Secondary affect is based on a more elaborate reflection, influenced by recollection, memory and anticipation, on the loss of autonomy and quality of life, the difficulties of enduring long-term pain, and the implications for the patient's future and survival. So chronic pain is often experienced not only as a threat to the current state of the body, comfort or daily activity, but also to future well-being and life in general.4
But what is the effect of cannabinoids on the affective component of pain? A meta-analysis of human laboratory studies, in which treatments are tested on healthy volunteers subjected to painful stimuli rather than on real patients, concluded that the administration of cannabinoid-based drugs prevented the onset of pain by producing small increases in pain threshold, but did not reduce the intensity of pain already being experienced. On the contrary, cannabinoids made the pain less unpleasant and more tolerable for the participants, suggesting an effect on the emotional processing of pain.5 In one of the experiments included in this meta-analysis, participants receiving THC in combination with morphine described a synergistic effect on the reduction of perceived discomfort, but not on pain intensity. The authors interpreted these two components using a simile with a radio: one dimension corresponds to the volume at which the radio is listened to, louder or quieter. The other corresponds to how annoying the radio is, which is a subjective value that is more qualitative than quantitative, and which may or may not be related to volume or intensity.6 This result is consistent with those obtained in observational studies of chronic patients receiving medical cannabis treatment, which report a small effect on perceived pain intensity, but a robust impact on health-related quality of life and a large improvement in psychiatric comorbidities such as mood, anxiety, stress or sleep quality.7
The memory of pain
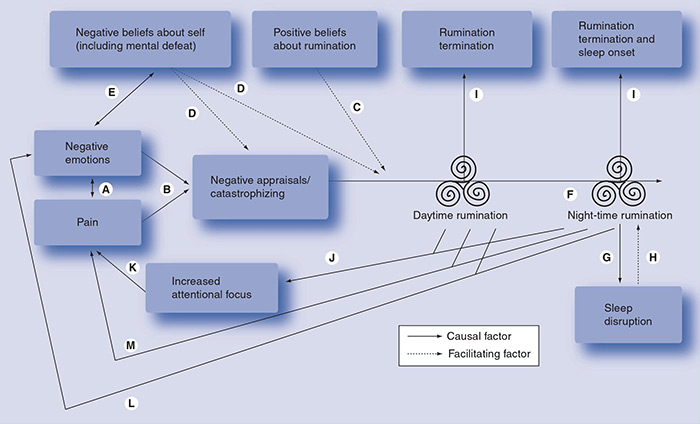
But how do cannabinoids selectively modulate the affective component of pain? Although the answer is not yet clear, we have some indications that come from neuroimaging studies in which participants are subjected to a painful stimulus. In these, it is observed that the administration of THC can block the increase of neuronal activity in the anterior cingulate cortex (ACC), a brain structure that is responsible for transferring painful information to higher nuclei where it is integrated with memories and experiences to elaborate affective responses. It is precisely this pathway that is lacking in lower animals such as rats, which produce a much more immediate and less processed response to painful stimuli.8 Similarly, we know that activation of cannabinoid receptor 1, the shared target of anandamide and THC, in another area of the brain called the amygdala, plays a key role in the extinction of aversive memories associated with negative or traumatic experiences. Experiences that are repeated are engraved in the memory, and continued painful experience generates a memory of pain. Fear and grief play a dominant role in the lives of chronic patients who live continuously with the expectation that pain will appear. Experts stress the importance of tackling this fear by generating pain-free spaces and thus developing a sense of control in the patient, which also contributes to reducing his or her general state of anxiety. Perhaps this could be one of the reasons why cannabinoids, through the control of the processing of the affective components of painful stimuli and the extinction of negative memories associated with chronic pain, could be more effective in those patients with psychiatric comorbidities such as stress, anxiety, and depression, which are the majority of patients suffering from chronic pain. The available evidence seems to indicate that the continued use of cannabinoids in this type of patients is able to improve behaviors such as catastrophizing and both day-time and night-time rumination, thus facilitating acceptance, resilience and positive thoughts about one's health (see figure).9
These brain areas, the ACC and the amygdala, are also implicated in the abnormal processing of aversive stimuli in psychiatric patients. Observational studies have identified a significant increase in communication between these two regions during fear-related emotional processes in patients diagnosed with anxiety disorders, but not in healthy volunteers. Moreover, this increased brain activity was positively correlated with anxious symptoms described by the patients.10 For this reason, cannabis-based medications may represent an effective addition to a multimodal pharmacological management plan not only for chronic pain, but also for other debilitating chronic conditions with a traumatic component such as anxiety disorders, such as social anxiety or generalized anxiety, or post-traumatic stress disorder.
A sigh of relief
But what does all this modulation of neuronal processes translate into for the patient? In qualitative studies in which the experience of patients who use cannabis for medicinal purposes is recorded, there are two recurring figures, common to most accounts: the first is the "sigh of relief", which is a figure of speech that patients commonly use to describe the effect they experience after inhaling cannabis. A feeling of bodily and mental relaxation that allows the patient to access a second sensation, that of "restoration of the self."11 Patients describe how the use of medical cannabis allows them to reconnect with themselves, with the person they were before they became ill, to carry out daily activities that gave them pleasure, such as taking care of their plants, taking a walk with their family or going out to dinner. In short, improving health-related quality of life, that delicate balance between fear of illness and love for one's own existence.
1. Huggins, J. P., Smart, T. S., Langman, S., Taylor, L. & Young, T. An efficient randomised, placebo-controlled clinical trial with the irreversible fatty acid amide hydrolase-1 inhibitor PF-04457845, which modulates endocannabinoids but fails to induce effective analgesia in patients with pain due to osteoarthritis of the knee. Pain 153, 1837-1846 (2012).
2. Di Marzo, V. Inhibitors of endocannabinoid breakdown for pain: not so FA(AH)cile, after all. Pain 153, 1785-1786 (2012).
3. Craig, A. D. A rat is not a monkey is not a human: Comment on Mogil (Nature Rev. Neurosci. 10, 283-294 (2009)). Nat. Rev. Neurosci. 10, 466 (2009).
4. Price, D. D. Psychological and Neural Mechanisms of the Affective Dimension of Pain. Science (80-. ). 288, 1769-1772 (2000).
5. De Vita, M. J., Moskal, D., Maisto, S. A. & Ansell, E. B. Association of Cannabinoid Administration With Experimental Pain in Healthy Adults: A Systematic Review and Meta-analysis. JAMA psychiatry 75, 1118-1127 (2018).
6. Roberts, J. D., Gennings, C. & Shih, M. Synergistic affective analgesic interaction between delta-9- tetrahydrocannabinol and morphine. Eur. J. Pharmacol. 530, 54-58 (2006).
7. Moreno-Sanz, G., Madiedo, A., Lynskey, M. & Brown, M. R. D. 'Flower Power': Controlled Inhalation of THC-Predominant Cannabis Flos Improves Health-Related Quality of Life and Symptoms of Chronic Pain and Anxiety in Eligible UK Patients. Biomed. 2022, Vol. 10, Page 2576 10, 2576 (2022).
8. Lee, M. C. et al. Amygdala activity contributes to the dissociative effect of cannabis on pain perception. Pain 154, 124-134 (2013).
9. Edwards, M. J., Tang, N. K., Wright, A. M., Salkovskis, P. M. & Timberlake, C. M. Thinking about thinking about pain: a qualitative investigation of rumination in chronic pain. http://dx.doi.org/10.2217/pmt.11.29 1, 311-323 (2011).
10. Robinson, O. J. et al. The dorsal medial medial prefrontal (anterior cingulate) cortexâ€"amygdala aversive amplification circuit in unmedicated generalised and social anxiety disorders: an observational study. The Lancet Psychiatry 1, 294-302 (2014).
11. Lavie-Ajayi, M. & Shvartzman, P. Restored Self: A Phenomenological Study of Pain Relief by Cannabis. Pain Med. 20, 2086-2093 (2019).


