By José Carlos Bouso

José Carlos Bouso is a clinical psychologist and a doctor of pharmacology. His areas of interest are psychopharmacology and the therapeutic properties of entactogens, psychedelics and cannabis. He has conducted therapeutic research with MDMA, pharmacological research with several substances of plant and synthetic origin and has also performed studies on the long-term neuropsychological effects of substances such as cannabis, ayahuasca and cocaine. He is author of the book "Qué son las drogas de síntesis" [What are synthetic drugs?], and co-author of “¿La marihuana como medicamento? Los usos médicos y terapéuticos del cannabis y los cannabinoides" [Marihuana as medicine? The medical and therapeutic uses of cannabis and cannabinoids] and "Ayahuasca y salud" [Ayahuasca and health]. His research has been published in scientific journals. He is currently the director of scientific projects at Fundación ICEERS.
Given the length of the article, it has been divided into three sections: the first part reviews the concept of addiction and sets out the different perspectives on tackling the phenomenon. The second part questions some of the axioms on which the biomedical science of addictions is based, namely that such addictions are due to the pharmacological effects of the drugs resulting from their ability to release dopamine in the brain. Finally, the third part of the article reviews the evidence from a variety of different studies (ethnographic, observational and clinical) on the potential use of cannabis in the treatment of drug dependence.
What is drug addiction?
The US National Institute on Drug Abuse, which sets the agenda for the rest of the world in determining the scientific position on drugs and drug addiction are, defines addiction in the following terms:
"Addiction is defined as a chronic, relapsing brain disease that is characterized by compulsive drug seeking and use, despite harmful consequences. It is considered a brain disease because drugs change the brain; they change its structure and how it works. These brain changes can be long lasting and can lead to many harmful, often self-destructive, behaviors."1
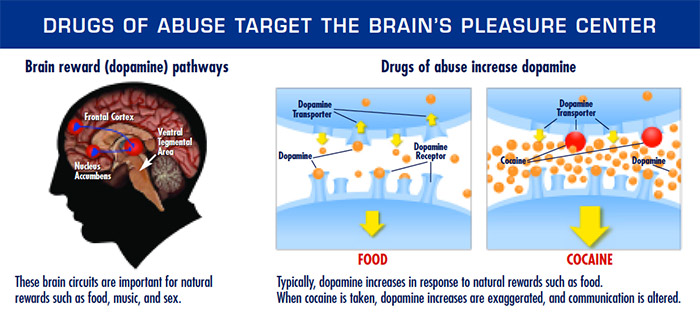
According to the NIDA’s theses –which are those that enjoy widest acceptance amongst by the scientific community, or at least those most widely used outside scientific circles– addiction occurs because the drugs act on what is known as the “reward circuit” (in its publications, the NIDA calls it the “pleasure centre”,2 a term which lacks any scientific meaning, as we shall discuss). The reward circuits are a series of neuronal pathways which are activated when someone feels motivated to perform a specific action in order to receive a reward that the body finds gratifying. Rewards may be biological –such as obtaining water, food or sex– or more culturally determined, such as winning a prize in the lottery or receiving some form of social recognition. When the organism initiates behaviour motivated by receiving a reward, a cerebral neurotransmitter called dopamine is released in the reward circuit. Dopamine is the substance that allows the organism to initiate and maintain reward-seeking behaviour (incidentally, dopamine is also released when the organism receives a punishment instead of a reward; this probably helps it to learn not to continue pursuing an erroneous goal). According to the NIDA ideologues, drugs cause addiction because they release more dopamine than “naturally” rewarding behaviours: “The effect of such a powerful reward strongly motivates people to take drugs again and again. This is why scientists sometimes say that drug abuse is something we learn to do very, very well”.
Naturally, this reductionist, overly biologistical vision of drug addiction is not shared by all scientists. Indeed, amongst all those professionally involved in studying and working with drugs, this notion is only shared by a section (fortunately not all) of the psychiatric profession, who need to present addiction as a type of disease in order to be able to prescribe pharmaceuticals to deal with it and promote their speciality as being just as worthwhile as any other medical speciality. What is curious is that, despite the fact that these theses have been accepted by a section of one part of the scientific community, and despite the billions of euros that have been invested in discovering a pharmaceutical that will “cure” drug addiction, not a single one has yet been found. Drug addiction appears to be a very elusive disease that resists pharmacological treatment. Indeed, there are studies showing that at least 80% of addicts quit drugs on their own with no need for external intervention.3 Interested readers will find a series of very well-founded criticisms of the concept of addiction-as-a-disease, based on scientific evidence, in the following publications:
- https://www.researchgate.net/publication/282211489_Que_es_y_que_no_es_la_adiccion_Evidencia_cientifica_disponible
- https://www.researchgate.net/publication/280876838_Salud_Mental_y_Adiccion
Revisiting the concept of addiction
The term “addiction” is derived from the Latin addicere, which means a strong inclination towards a good or bad practice. In the early nineteenth century, the term began to take on pejorative connotations and be used to refer to morbid appetites, socially deviant habits and vicious behaviour. The first time the term was used to refer to the consumption of a drug was in relation to coffee. Coffee has probably been the most vilified drug in history. In different cultures and at different times, it has been banned and legalized. In Tsarist Russia coffee addicts were severely punished. Yet despite the moral and physical harm caused by the vice, not to mention the dramatic consequences if they were caught by the police, consumers continued to frequent clandestine coffee houses where they could compulsively take their drug of choice. It is clear evidence that drug addiction has a strong social component and is strongly influenced by the drug policies of the age, more than by biology and disease. In the case of coffee, this situation strikes us today as absurd; yet it is closely echoed in the modern world by the situation of illegal drugs; indeed there are even countries, such as the Philippines, where the newly elected president has lent his support to the summary execution of drug takers, leaving nearly two thousand dead since last July.4 To return to the history of the concept of addiction and drugs, at the beginning of the twentieth century the term began to be used to refer to alcohol and by the middle of the century it was extended to include all drugs.5
Today, however, science has gradually abandoned the term "addiction" in favour of the vaguer and more ambiguous term, “drugs of abuse”. The method used to define drugs of abuse is as follows: subjects are given the drug in a laboratory context and then asked to complete a questionnaire: if they tick the boxes “I like this pharmaceutical” and “I would repeat the experience”, then it is a drug of abuse. Literally. The criterion for classing a substance as a drug of abuse is that people like its effects. Tolerance, physical dependence, withdrawal symptoms and compulsive consumption are no longer considered necessary criteria for diagnosing “substance abuse”, according to common nosological classifications (DSM-5). The diagnosis refers exclusively to the harmful consequences of consumption. The problem with this definition is that the harmful consequences are highly conditioned, as we have already seen, not so much by the pharmacology of the substances (although that is also a factor), but probably more by the socio-political context in which they are framed.6 In this context, there should be a psychiatric diagnosis along the lines of "Abuse of public policies” and such policies should be termed “policies of abuse” – and that includes public policies on tobacco and alcohol. For example, it is striking that so many of the sports events that attract the largest national audiences are sponsored by brands of beer. And the Spanish National Drugs Plan (the PNSD) bestowed the White Cross of the Order of Merit on the association of manufacturers of alcoholic beverages for their "efforts" in combatting abusive consumption and permissiveness in sales to minors.7 Maybe reality is a hallucinogenic?
1. https://www.drugabuse.gov/publications/media-guide/science-drug-abuse-addiction-basics
2. https://www.drugabuse.gov/publications/drugs-brains-behavior-science-addiction/drugs-brain
Heyman, GM. 2013. Quitting drugs: quantitative and qualitative features. Annual Review of Clinical Psychology. 9:29-59. Lopez-Quintero C, Hasin DS, de los Cobos JP, Pines A, Wang S, Grant BF, Blanco C. 2011. Probability and predictors of remission from life-time nicotine, alcohol, cannabis or cocaine dependence: Results from the national epidemiologic survey on alcohol and related conditions. Addiction. 106(3): 657-669.
4. http://internacional.elpais.com/internacional/2016/08/23/actualidad/1471947959_120093.html
5. Frenk H, Dar R. 2000. A critique of nicotine addiction. Boston: Kluwer Academic Publishers.
6. For an in-depth analysis of this idea see: Bouso JC: El sesgo legal en el estudio neuropsicológico de la adicción. In: J.M. Ruiz Sánchez de León, E.J. Pedrero Pérez: Neuropsicología de la Adicción. Madrid: Editorial Médica Panamericana.
7. http://www.infolibre.es/noticias/politica/2016/05/23/el_plan_nacional_sobre_drogas_premia_patronal_bebidas_alcoholicas_50133_1012.html


